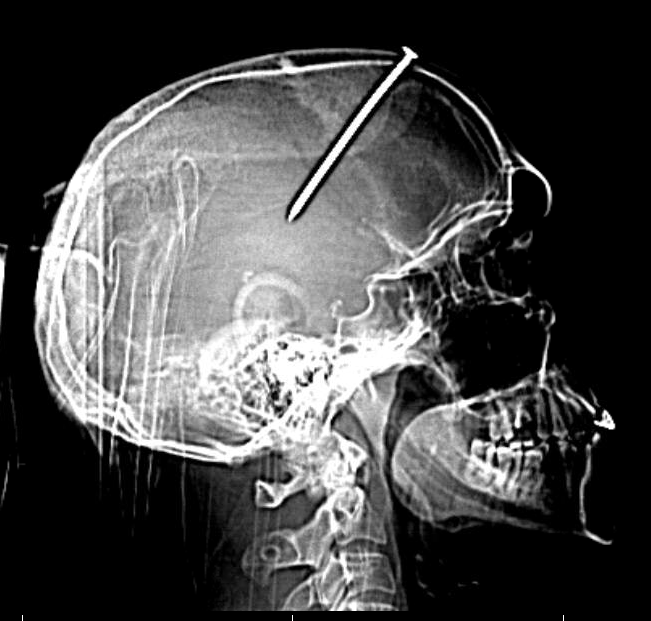
Awake adult presents after workplace nail gun accident
What’s the diagnosis?
Left frontal penetrating trauma due to nail gun deployment. Prior to nail removal there is no obvious injury to the intracranial arteries on the CT angiogram or formal angiographic runs, although the nail trajectory is in close proximity to the anterior cerebral arteries as they wrap around the corpus callosum. After nail removal there is new hemorrhage along the nail tract and within the ventricles causing hydrocephalus. On subsequent angiography the right anterior cerebral artery, pericallosal segment, demonstrates a traumatic pseudoaneurysm.
Background
Penetrating cerebrovascular injuries are rare events. Penetrating trauma can lacerate an intracranial artery forming a traumatic pseudoaneurysm. In a traumatic pseudoaneurysm, the aneurysm walls are actually formed by surrounding tissues and not vessel wall.
Penetrating trauma mechanisms that lead to traumatic pseudoaneurysms are typically low velocity, such as stab wounds, as opposed to high velocity penetrating trauma (e.g., gun shot wounds).
What's your treatment plan?
The patient is developing acute hydrocephalus from intraventricular hemorrhage. An external ventricular drain should be placed to normalize intracranial pressure.
A ruptured distal pericallosal aneurysm could be treated with an endovascular approach, such as embolization. Alternatively, an parasagittal interhmispheric open microsurgical approach could be used to clip this aneurysm.
In this case, because of the hemorrhage noted on the post nail removal CT head scan the patient immediately returned to the angiography suite. The distal right anterior cerebral artery, pericallosal segment, traumatic pseudoaneurysm was identified. A microcatheter was advanced into the right ACA and brought just proximal to the aneurysm. Onyx liquid embolization material was used to occlude the pericallosal vessel both distal and just proximal to the aneurysm, to eliminate the risk of further hemorrhage.
The microcatheter was advanced into the distal pericallosal branch and a gentle injection through the microcatheter was used to confirm its location just proximal to the traumatic pseudoaneurysm.