Octogenarian with waxing and waning right body hemiparesis suddenly develops severe aphasia and right hemiplegia
What’s the diagnosis?
Complete left internal carotid artery occlusion just distal to the left common carotid artery bifurcation. There is reconstitution of the left internal carotid artery at the level of the ophthalmic segment via flow from the external carotid artery retrograde through the ophthalmic artery.
There appears to be an occlusion of the left middle cerebral artery at the M1 segment because even when collateral flow fills the left supraclinoid internal carotid artery, there is no filling of the MCA branches distal to the very proximal M1 segment.
There is modest collateral flow to the left cerebral hemisphere from the left posterior cerebral artery and from the right anterior cerebral artery through leptomeningeal, or pial collaterals.
Background
Patients with a chronically occluded internal carotid artery have an ↑ risk of ischemic events in the ipsilateral hemisphere, about 5% per year.
In the setting of an occluded internal carotid artery, patients typically depend on collateral circulation to prevent stroke, or infarction in the brain that would have normally been fed by the occluded carotid artery. To augment their collateral circulation, these patients are typically chronically hypertensive.
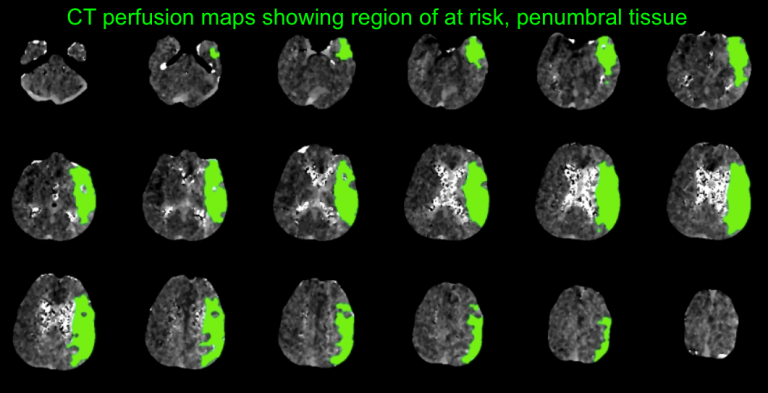
Preoperative testing includes imaging studies that document complete occlusion of the internal carotid artery, such as CT angiography. Perfusion imaging is useful to document ipsilateral hemispheric hypoperfusion.
A complete diagnostic angiogram should be performed to determine whether or not there is any collateral flow to the ipsilateral internal carotid artery distal to the occlusion. For example, in this case the ipsilateral external carotid artery → ophthalmic artery → retrograde filling of the ophthalmic segment of the internal carotid artery. This endoluminal flow in the internal carotid artery distal to the occlusion site implies lumen patency and documents a potential target landing zone to reach if revascularization is going to be attempted.
What's your treatment plan?
This disease process has been studied extensively and several treatment approaches have not shown a survival benefit. For example, both carotid endarterectomy and superficial temporal artery-to-middle cerebral artery bypass have been studied in clinical trials of high-risk stroke patients but have not shown significant benefits.
Endovascular treatment with revascularization is technically feasible in some patients, but there are risks to reopening the occluded carotid artery. Distal embolization of clot that has formed in the occluded vessel could → stroke. Vessel perforation, iatrogenic pseudoaneurysm, and the creation of a fistula between the carotid artery and surrounding venous structures are serious possibilities. And, once the vessel is re-opened, cerebral hyperperfusion must be avoided.
During this procedure, blood pressure management is critically important. A reliable arterial line should be obtained for accurate blood pressure monitoring. Before the carotid artery is opened, patients are typically severely hypertensive. It is important to avoid lowering their blood pressure with sedating medications (or general anesthesia) because this relative blood pressure decrease could cause the at-risk tissue to stroke completely, or infarct. Once the artery is opened, patients typically drop their blood pressure significantly as their brain attempts to prevent reperfusion, or hyperperfusion injury. It is important to avoid profound systemic hypotension during this period because they could develop cerebral or systemic hypoperfusion and end-organ damage. If needed, patients can be supported with intravenous vasopressors.
In this case, because the patient showed significant clinical worsening that correlated with a large left hemispheric at risk territory, the decision was made to attempt revascularization of the occluded left internal carotid artery. This was achieved by developing a channel through the occluded internal carotid artery, deploying a distal embolic protection device, and placing a stent in the extracranial internal carotid artery at the level of the carotid bifurction. The distal embolic protection device was removed. A left MCA M1 segment thrombectomy was performed with manual aspiration and anterograde perfusion through the left MCA was restored.
The ICA stump site is probed with a microwire and microcatheter.
If the occlusion is transgressed, the microwire and catheter should be advanced until a patent segment of the ICA is reached.