Middle-aged adult with sudden loss of consciousness at home, intubated at nearby hospital, now with non-reactive pupils and extensor, decerebrate posturing
What’s the diagnosis?
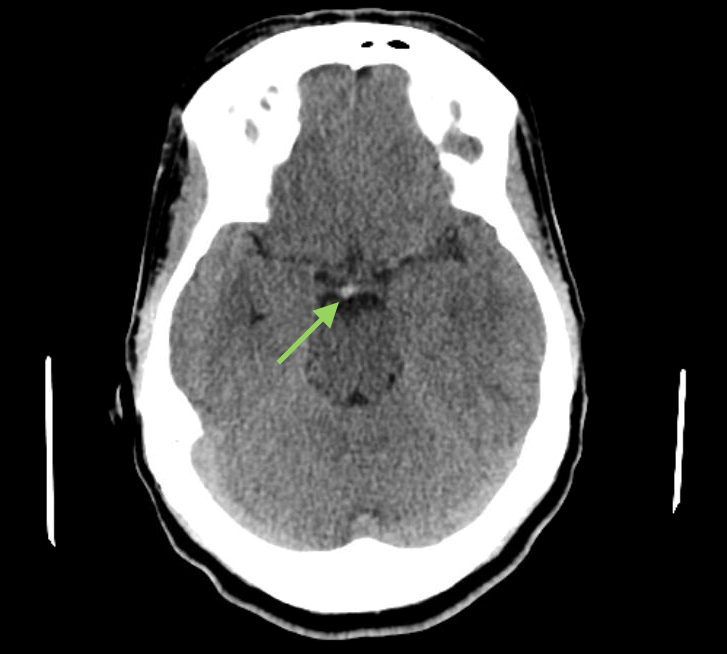
There is an acute basilar artery occlusion. The CT head shows a focal hyperdensity at the basilar apex, concerning for acute embolus. Arteriography demonstrates occlusion of the basilar artery.
Note the hyperdense basilar artery sign on the CT head non contrast scan.
Background
Basilar artery occlusion is a rare cause of sudden loss of consciousness. Left untreated, basilar artery occlusion → mortality rate of >80%.
A hyperdense artery sign is caused by the ↑ hematocrit concentration of embolus or thrombus. Clot has a ↓ plasma concentration and ↑ red blood cell concentration. For example, the attenuation of flowing blood is <40 Hounsfield units but the attenuation of hematocrit-dense clot is often >80 Hounsfield units. This explains why clot looks hyperdense on CT scans.
The hyperdense middle cerebral artery sign is a well known radiographic finding on CT scans. It is especially powerful because the ipsilateral middle cerebral artery appearance can be compared to the contralateral, normal middle cerebral artery appearance.
The hyperdense basilar artery sign can indicate acute embolus within the basilar artery. However its usefulness as a radiographic finding may be limited because there is often significant streak artifact within the posterior fossa on CT scans and because there is no comparable (paired) contralateral artery against which to evaluate symmetry.
Therefore, the hyperdense basilar artery sign is most useful in the context of a patient with clinical signs and symptoms consistent with basilar artery occlusion, such as ↓ consciousness, cranial nerve palsies, quadriparesis, and primitive posturing.
What's your treatment plan?
Restoration of blood flow through the basilar artery should be achieved as quickly as possible.
In the setting of basilar artery occlusion, patients may require basic supportive measures such as endotrachial intubation.
Emergent endovascular intervention is indicated.
In this case, endovascular manual aspiration embolectomy was performed, which achieved reperfusion of the basilar artery and restored flow through the posterior circulation.
Following endovascular embolectomy there is complete reperfusion of the basilar artery and flow is restored.