Middle aged adult presents with acute onset worst headache of life
What’s the diagnosis?
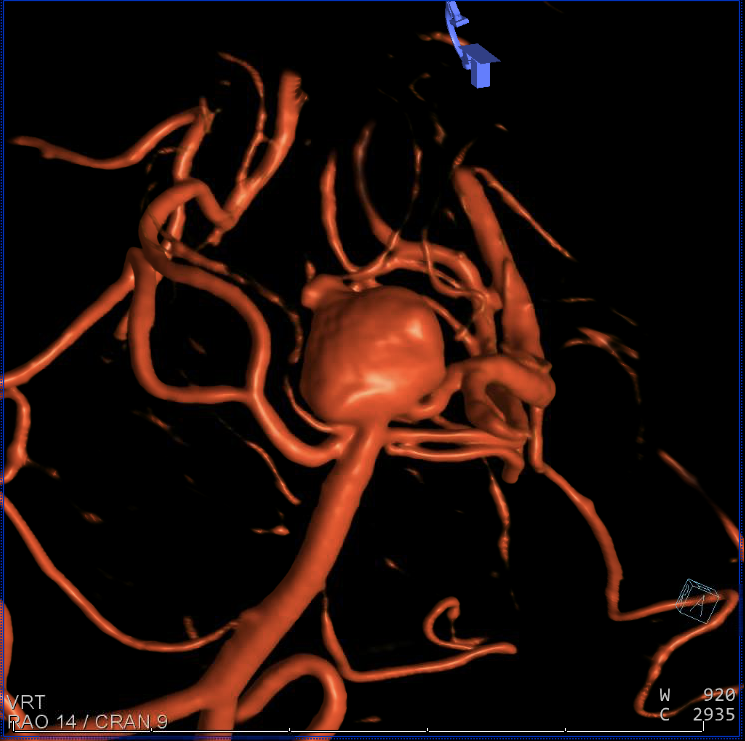
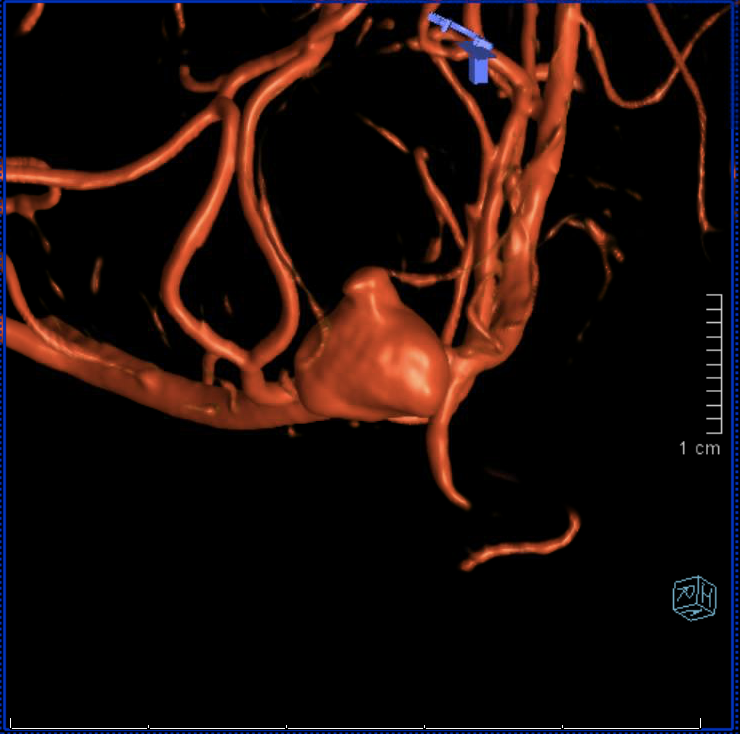
Ruptured 10 mm superiorly-projecting basilar apex aneurysm with an irregular 3 mm rightward-pointing daughter sac. The neck of the aneurysm incorporates the left posterior cerebral artery origin and the right superior cerebellar artery origin. There is a fetal right PCOMM artery and a hypoplastic right posterior cerebral artery P1 segment.
Background
The term “fetal” posterior communicating (PCOMM) artery refers to a PCOMM that is larger than the posterior cerebral artery P1 segment. It implies that the majority of blood flow to the posterior cerebral artery P2, P3, and P4 segments comes via flow from the anterior circulation through the large PCOMM artery, as opposed to through the posterior circulation through the diminutive P1 segment.
In this case, the large right PCOMM artery feeds the right posterior cerebral artery territory. The right posterior cerebral artery P1 segment is hypoplastic, and there is therefore no physiological reason to spare it while treating this aneurysm.
In the setting of acutely ruptured intracranial aneurysms, the use of adjunctive endovascular devices that require dual antiplatelet therapy such as endovascular stents is often avoided because dual antiplatelet therapy may → ↑ adverse events like intracranial hemorrhage, ventriculostomy-related hemorrhages, and difficulty if the patient needs subsequent open surgery.
In this case, the aneurysm neck incorporates the origins of both the left posterior cerebral artery and the right superior cerebellar artery, but there is no way to completely coil embolize the aneurysm neck without jeopardizing the patency of these exiting vessels. It may be reasonable to place a protective device, such as an endovascular stent from the right SCA to the left PCA P1 segment in the future when the patient is able to tolerate dual antiplatelet therapy, if the neck requires further coil embolization.
What's your treatment plan?
Management options for ruptured intracranial aneurysms include open surgical clip reconstruction and endovascular embolization.
In this case, coil embolization of the ruptured basilar apex aneurysm was performed. A balloon was placed from the basilar artery into the left posterior cerebral artery P1 segment to protect the PCA origin from any coil prolapse. A two-catheter coiling technique was used to sequentially entangle framing and then filling coils about one another. The objective was to "dome coil" embolize the aneurysm dome but leave patent the aneurysm neck that incorporated the left PCA and right SCA origins.