Elderly adult severe headache 1 week ago. Lost consciousness at home today. Now drowsy with right eye ptosis and pupillary dilation
What’s the diagnosis?
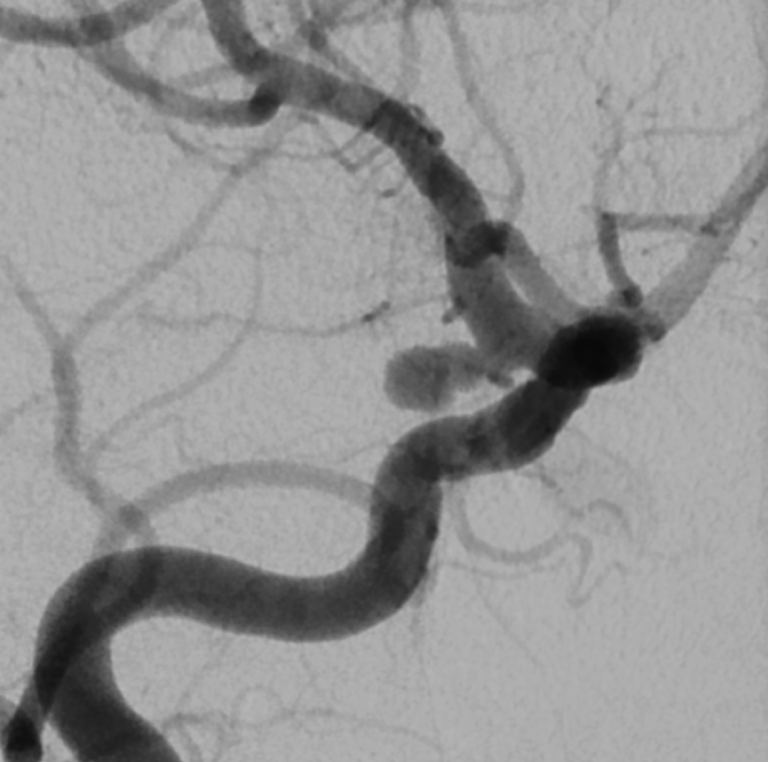
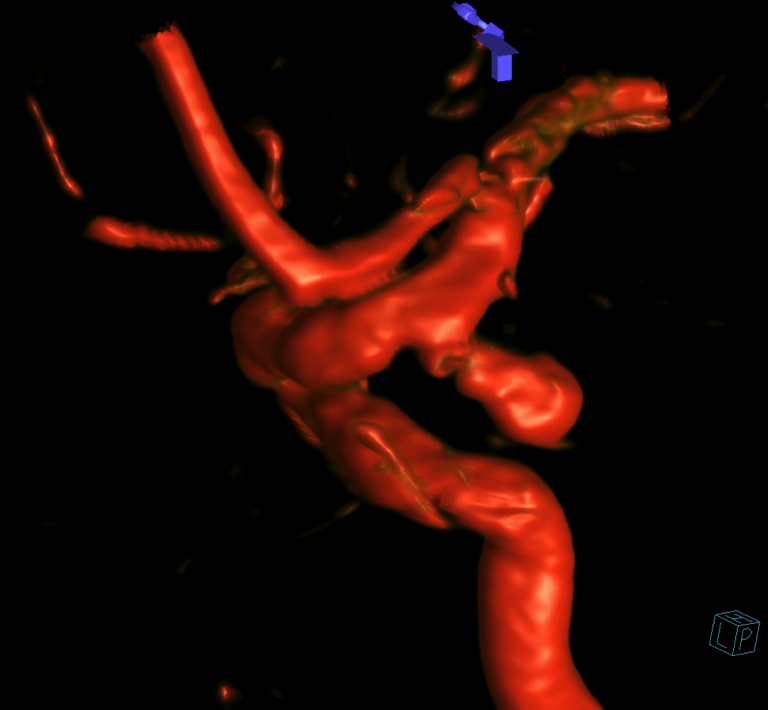
Ruptured, right posterior communicating artery aneurysm causing an acute subdural hematoma, subarachnoid hemorrhage, and also an oculomotor nerve palsy
Differential Diagnosis
Ruptured right posterior communicating artery aneurysm
Other, more common causes of spontaneous subdural hematoma include trauma and coagulopathy
Background
Although uncommon, acute subdural hematoma due to aneurysmal rupture is a well known radiographic presentation, most commonly seen with ruptured posterior communicating artery aneurysms.
Manual compression of the oculomotor nerve by posterior communicating artery aneurysms may → oculomotor nerve palsy (e.g, diplopia, ptosis, opthalmoplegia, pupillary dysfunction)
In patients with ruptured PCOM aneurysms it appears that microsurgical clipping may afford a better chance of oculomotor nerve palsy improvement than endovascular coiling.
What's your treatment plan?
Treatment options for ruptured posterior communicating artery aneurysms include endovascular coil embolization and microsurgical clip reconstruction.
In this case the patient had an acute subdural hematoma ipsilateral to the ruptured aneurysm that was causing right-to-left midline shift. She also had right-sided oculomotor nerve palsy.
Open craniotomy was felt to offer both evacuation of the acute subdural hematoma as well as microsurgical clip reconstruction of the ruptured aneurysm.
In this case, a right-sided craniotomy was performed with evacuation of the subdural hematoma and microsurgical clip reconstruction of the ruptured right posterior communicating artery aneurysm.