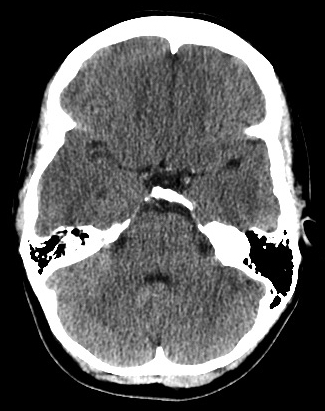
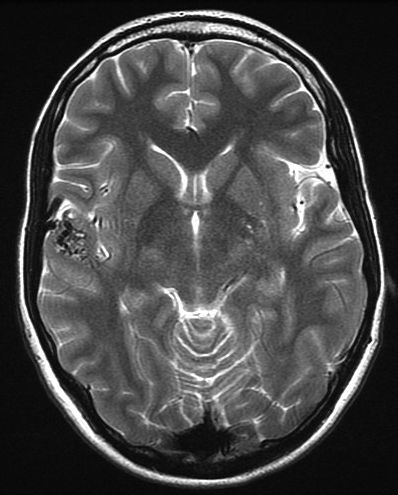
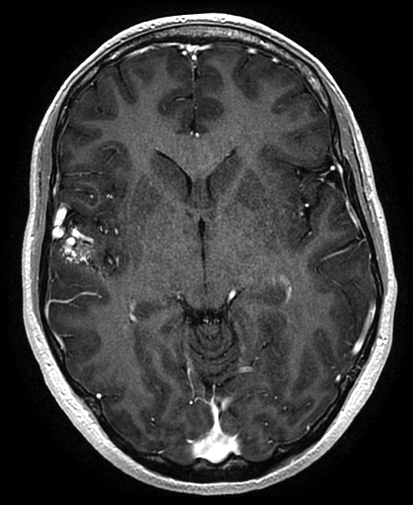
Young adult intact neurological exam, subjective right facial paresthesias
What’s the diagnosis?
Unruptured, Spetzler-Martin grade 1 right temporal arteriovenous malformation supplied by middle cerebral artery feeders and drained by a frontal cortical vein. There are no obvious high-risk features such as deep location, exclusively deep venous drainage, or associated aneurysm.
Background
The Spetzler-Martin grading scale for arteriovenous malformations of the brain was developed to predict the outcome of microsurgical treatment and is widely used to describe these malformations.
This five-grade scale incorporates points for three important features of an arteriovenous malformation: 1) the largest diameter of the nidus of the malformation as measured on angiography; 2) the presence of deep venous drainage (e.g., the internal cerebral veins, basal veins, or precentral cerebellar vein); and 3) eloquent location (e.g., motor, sensory, language, and visual cortex or basal ganglia).
The general microsurgical strategy is to first cauterize feeding arteries and then draining veins. The goal is complete removal of the malformation as a single specimen.
For Spetzler-Martin grade 1 or 2 arteriovenous malformations, the risk of new, permanent neurological deficits after microsurgery is felt to be less than 5% amongst experienced surgeons.
However, the risk of neurological injury increases dramatically with higher grade arteriovenous malformations.
What's your treatment plan?
In general, treatment options for brain arteriovenous malformations include observation, microsurgical resection, radiosurgery, and endovascular embolization.
In this case, the arteriovenous malformation nidus is less than 3 cm (1 point), located in non-eloquent tissue (0 points), and has superficial venous drainage (0 points), meaning that it is a Spetzler-Martin grade 1 lesion.
Because the patient is young, her cumulative lifetime risk of rupture is relatively high.
In this case, a right-sided craniotomy and microsurgical resection of the arteriovenous malformation was performed. An intraoperative angiogram was performed as well to confirm complete obliteration of the lesion.