Elderly adult with 1 week of double vision, found to have a partial left-sided oculomotor nerve palsy
What’s the diagnosis?
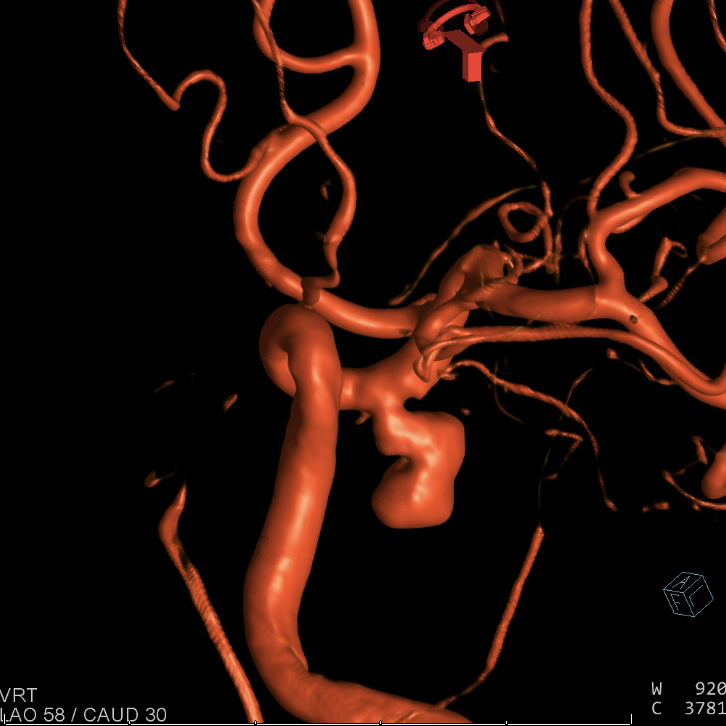
There is an unruptured, bilobed, 1 cm left posterior communicating artery aneurysm without any significant exiting branch artery. This aneurysm is newly symptomatic and is causing an ipsilateral partial oculomotor nerve palsy.
Background
There are many different possible causes of new-onset ophthalmoplegia, or restricted ocular movement.
One important potential neurovascular cause of an oculomotor nerve (cranial nerve 3) palsy is irritation of the oculomotor nerve at its cisternal segment by a posterior communicating (PCOMM) artery aneurysm.
The precise pathophysiology of this “irritation” is poorly understood. Some argue it is related to direct aneurysmal mass effect on and mechanical compression of the oculomotor nerve. Others believe it is arterial pulsations of the aneurysm that irritate the neighboring oculomotor nerve.
When a PCOMM artery aneurysm ruptures and causes subarachnoid hemorrhage, emergent treatment is necessary to secure the aneurysm and prevent recurrent hemorrhage. However, in the case of unruptured PCOMM artery aneurysms that cause new-onset ophthalmoplegia, it is felt that some change in the shape or behavior of the aneurysm must be occurring to cause these new symptoms. Aneurysms that are “changing” are believed to be higher risk for impending rupture.
What's your treatment plan?
For ruptured posterior communicating (PCOMM) artery aneurysms, treatment with microsurgical clip reconstruction is superior to endovascular coil embolization, with regard to improvement of an oculomotor nerve palsy.
For unruptured PCOMM artery aneurysms, it is unclear whether clipping or coiling is superior, with regard to improvement of an oculomotor nerve palsy.
Flow diversion of symptomatic, unruptured PCOMM artery aneurysms may be a useful alternative treatment strategy. Over time, flow diversion → ↓ aneurysm size and thus ↓ aneurysmal mass effect on the oculomotor nerve. And, flow diversion alters blood flow into the aneurysm, which → ↓ arterial pulsations of the aneurysm that irritate the oculomotor nerve.
The pipeline embolization device is an endovascular flow diverter that redirects blood flow down the axis of the vessel. Although flow diverters immediately reduce the blood flow into an aneurysm they do not immediately eliminate it. For this reason, a combination of 1 or 2 coils — which promote immediate thrombosis within the aneurysm — and placement of a pipeline device across the aneurysm neck may be performed in a single setting.
In this case, although the aneurysm was unruptured, the onset of new ophthalmoplegia was interpreted to be a warning sign that the aneurysm was changing and could possibly rupture in the near future. For this reason and also in an attempt to improve the disabling oculomotor nerve palsy, treatment was performed. Endovascular “loose” coiling of the aneurysm was performed with a single coil to promote endosaccular thrombosis of the aneurysm dome. Pipeline embolization device flow diversion was performed across the aneurysm neck.